



What?! Anomalous Coronary Arteries Seen with Echo
A Closer Look

Background
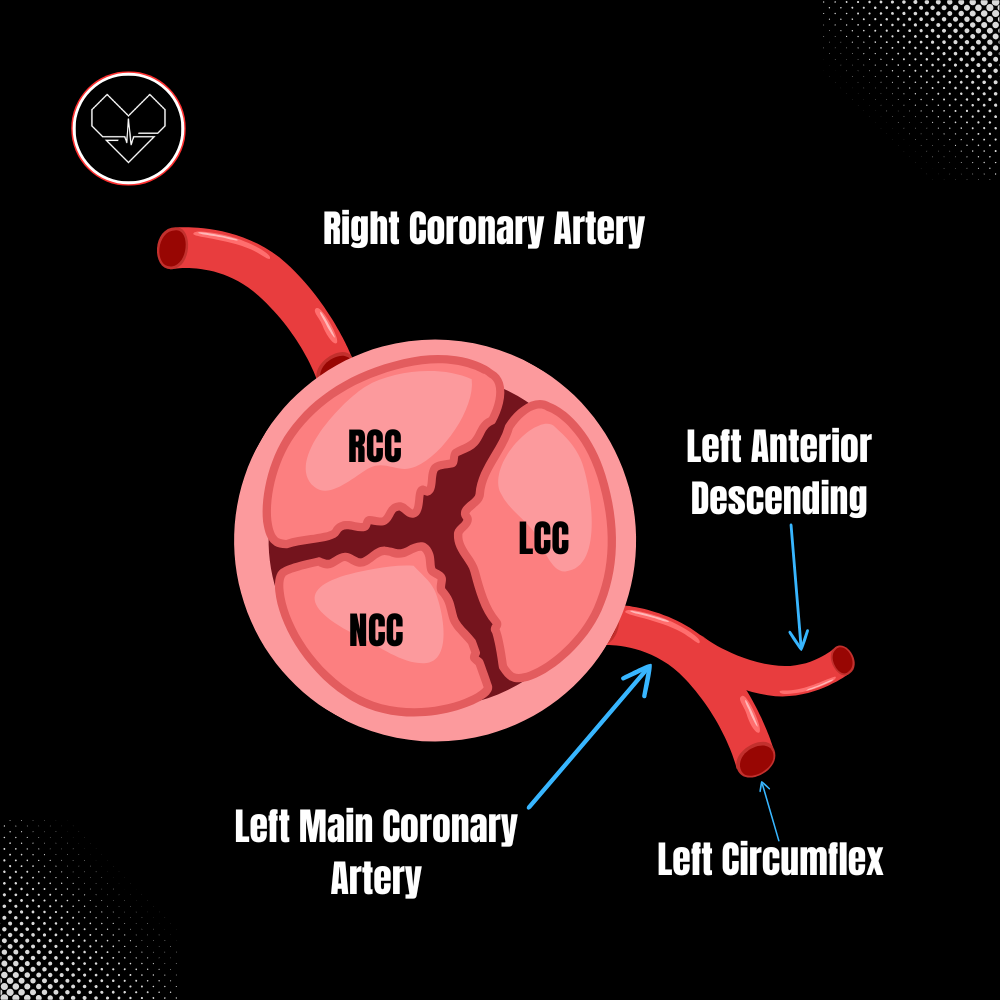
While we typically tell patients that we can’t visualize coronary arteries with echocardiography due to their size, today's lesson reveals rare and abnormal cases where abnormal coronaries are seen on TTE. In normal anatomy, the left main coronary artery (LMCA) and the right coronary artery (RCA) arise from the aortic sinuses and come together towards the apex of the heart. The LMCA supplies oxygenated blood to 2/3 of the interventricular septum and splits into the left anterior descending (LAD) and left circumflex artery (LCX) whereas the RCA supplies blood to the remaining 1/3.
In about 1.3% of patients, the coronary artery morphology is considered anomalous, or irregular and unusual. In today’s lesson for premium members, we will explore how echocardiography can reveal the RAC sign (retroaortic anomalous coronary sign) or the Bleb sign, suggesting an anomalous LCX pathway.
Introduction
The increased use of echocardiography and advanced coronary imaging in adults has led to more frequent identification of coronary artery anomalies (CAAs), often as incidental findings. However, the prognostic implications of CAAs are not well understood, and treatment decisions are based on limited evidence. Managing asymptomatic patients, especially younger individuals, can be challenging. CAAs are linked to an increased risk of sudden cardiac death (SCD), particularly in young athletes, where anomalous coronary origins are the second most common cause of SCD in competitive sports (AHA, 2021).
The diagnosis is typically straightforward with coronary angiography (CA) or computed tomography, but coronary anomalies may be seen on transthoracic echocardiography (TTE). Both RAC sign and Bleb sign can suggest that the left circumflex travels behind the aorta; here are the expert imaging techniques and key characteristics to look for.