

Pulmonary Embolism: Types, Case Studies, and the Role of Echocardiography
Everything You Need to Know

Role of Echocardiography
According to medical consensus, a pulmonary embolism (PE) is the third most common cause of cardiovascular death in the United States, following myocardial infarction and stroke. As cardiac sonographers, we can use echocardiography to assess right ventricular dilation and dysfunction, right heart strain, morphology of the interventricular septum, pulmonary hypertension, and hemodynamic instability (AHA, 2024).
A thrombus can be visualized anywhere in the inferior vena cava, superior vena cava, right atrium, right ventricle, or pulmonary artery before it reaches the lungs.
What is it?
A pulmonary embolism (PE) occurs when a blood clot blocks a vessel in the lungs, disrupting flow and oxygen exchange. This condition is a medical emergency that requires immediate diagnosis and treatment. A PE can occur in an acute, subacute, or chronic setting. According to the Cleveland Clinic, about 1/3 of patients with a pulmonary embolism die before they are able to get a diagnosis and treatment.
Blood stagnation (pooling) can occur in the arms or legs after long periods of inactivity; some examples include bed rest, long plane rides, or inactivity after surgery. Furthermore, an injury to a vein from a fracture or surgery can also increase the risk of emboli development in the pelvis, hip, knee, or leg. Pre-existing cardiovascular diseases such as heart failure, atrial fibrillation, heart attack, or stroke are also risk factors for PE (Cleveland Clinic, 2024). The above case displays a critical echo finding, a highly mobile and large right atrial thrombus protruding through the tricuspid valve during diastole.
Key Echo Findings
Right ventricular size & function
Echocardiography is used to quantify the size and the function of the right ventricle in a focused view. A lateral apical image is preferred for linear RV dimensions and fractional area change (FAC), if the acoustic window is available. Tricuspid annular plane systolic excursion and tissue Doppler index (TDI) should be measured in an on-axis view so that the annular motion towards the apex is accurately assessed.
When the right heart is dilated and overloaded, the interventricular septum is important to note; pressure and volume overload change the morphology and behavior. The first clip shows the interventricular septum flattening throughout the cardiac cycle as right heart pressures exceed left heart pressures - this is called a “D-shaped septum”. Moreover, we can then appreciate the interatrial and the interventricular septum bowing towards the left heart in the apical 4-chamber view that follows.
Right heart strain
Right heart strain is defined as pressure or volume overload of the right ventricle that leads to hemodynamic compromise. Some common causes for this include of chronic lung disease, pulmonary hypertension, left heart failure, arrhythmogenic right ventricular dysplasia, RV infarct, sleep apnea, or in this case pulmonary embolism.
McConnell’s sign is an echocardiographic characteristic indicating right ventricular dysfunction, featuring hypokinesia of the basal to mid portions of the free wall and hyperdynamic motion of the apex. This has proved to be highly specific for acute pulmonary embolism but is not seen in every case. Off-axis images are highly recommended to further investigate the apex’s hyperdynamic motion.
Cor Pulmonale
Ultimately, right heart strain can lead to cor pulmonale, a lung issue that causes right heart failure and dilation. High pulmonary pressures make it difficult for the right ventricle to pump adequate blood into pulmonary circulation; echocardiography is serially used to assess the right ventricular systolic pressure (RVSP). Cor pulmonale can occur acutely due to a pulmonary embolism or over an extended period of time in the presence of COPD, ventilator injury, cystic fibrosis, obstructive sleep apnea, or other lung conditions.
Echo is used to monitor right ventricular size, function, and pulmonary pressures. Be sure to thoroughly investigate the peak tricuspid regurgitant velocity and the collapsibility of the inferior vena cava (m-mode with sniff) to accurately quantify right ventricular systolic pressures.
Saddle Pulmonary Embolism
A saddle pulmonary embolism is a rare type of acute PE where a large blood clot blocks the bifurcation of the pulmonary artery, restricting blood flow to both lungs. This is typically a larger and more unstable thrombus and accounts for about 2-5% of all pulmonary embolism cases (Healthline, 2021). There is an increased risk of embolization with this type of PE, traveling further down into the right and left pulmonary arteries, or other branches of the lungs.
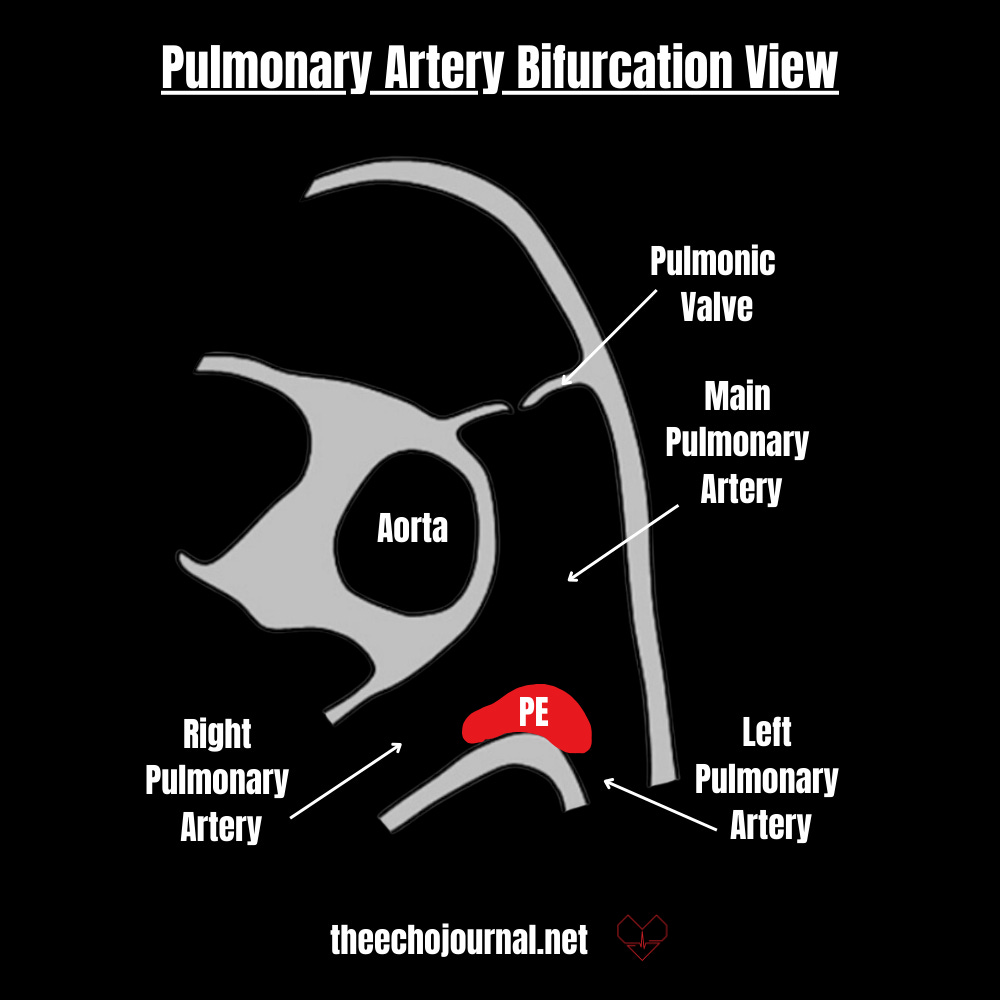
The term “saddle” is used because the clot fastens atop the main pulmonary artery where it branches into the right and left pulmonary artery, similar to a horse saddle. Symptoms can vary greatly depending on the size of the clot, how much lung is involved, and any coexisting lung or cardiovascular conditions. Shortness of breath and worsening chest pain upon inspiration are some of the more common symptoms seen in cases of PE.
The first example above displays a classic saddle pulmonary embolism whereas the second case, “PA Thrombus", shows a mobile clot in the main pulmonary artery in both the long axis and bifurcation view. This echogenic structure is seen floating in the mid portion of the pulmonary artery and has a high risk of embolization to the lungs, resulting in a pulmonary embolism.
Right Ventricular Thrombus
A right heart thrombus is an uncommon but serious form of venous thromboembolic disease that can be found along with pulmonary emboli. They often originate from deep vein thrombosis but can get stuck “in transit” to the lungs - this clot adhered to the right ventricular free wall as indicated in the below case along with McConnell’s sign. These clots can also form as a result of heart failure, ventricular dysfunction, atrial fibrillation, implantable devices, catheters, or even prosthetic valves.
Summary
Echocardiography plays a key role in assessing the hemodynamic complications of pulmonary embolism, offering valuable functional insights into the right heart that are not achievable by other modalities.
Right ventricular size & function - Measure, TAPSE, TDI, FAC
Right heart strain - McConnell’s sign, septal flattening or bowing, right heart enlargement
Pulmonary hypertension -right ventricular systolic pressures (close attention to peak TR & IVC collapsibility), keep cor pulmonale in mind
Enjoyed this lesson?
Join our international community of echo professionals and get fresh lessons delivered straight to your inbox every Tuesday and Thursday. Don't miss a beat—sign up today for the full experience.
