

Abdominal Aortic Dissection
Detection with Echocardiography

Background
The Cleveland Clinic reports that abdominal aortic aneurysms (AAA) are more prevalent than thoracic aortic aneurysms, affecting 1.1 million individuals in the U.S. aged 50 to 84. Detection can be difficult as aortic aneurysms often grow over time and don’t always cause symptoms; those that report symptoms typically complain of deep pain in stomach area, back pain, or a pulse near the belly button.
Aneurysms can occur anywhere along the aorta but most occur in the abdominal portion (75%) as a result of atherosclerosis, hypertension, trauma, or in rare cases infection. This diagnosis predominately affects patients over the age of 65 and is four times more common in people assigned male at birth. Smoking is a considerable risk factor as it weakens blood vessel walls (Cleveland Clinic, 2024).
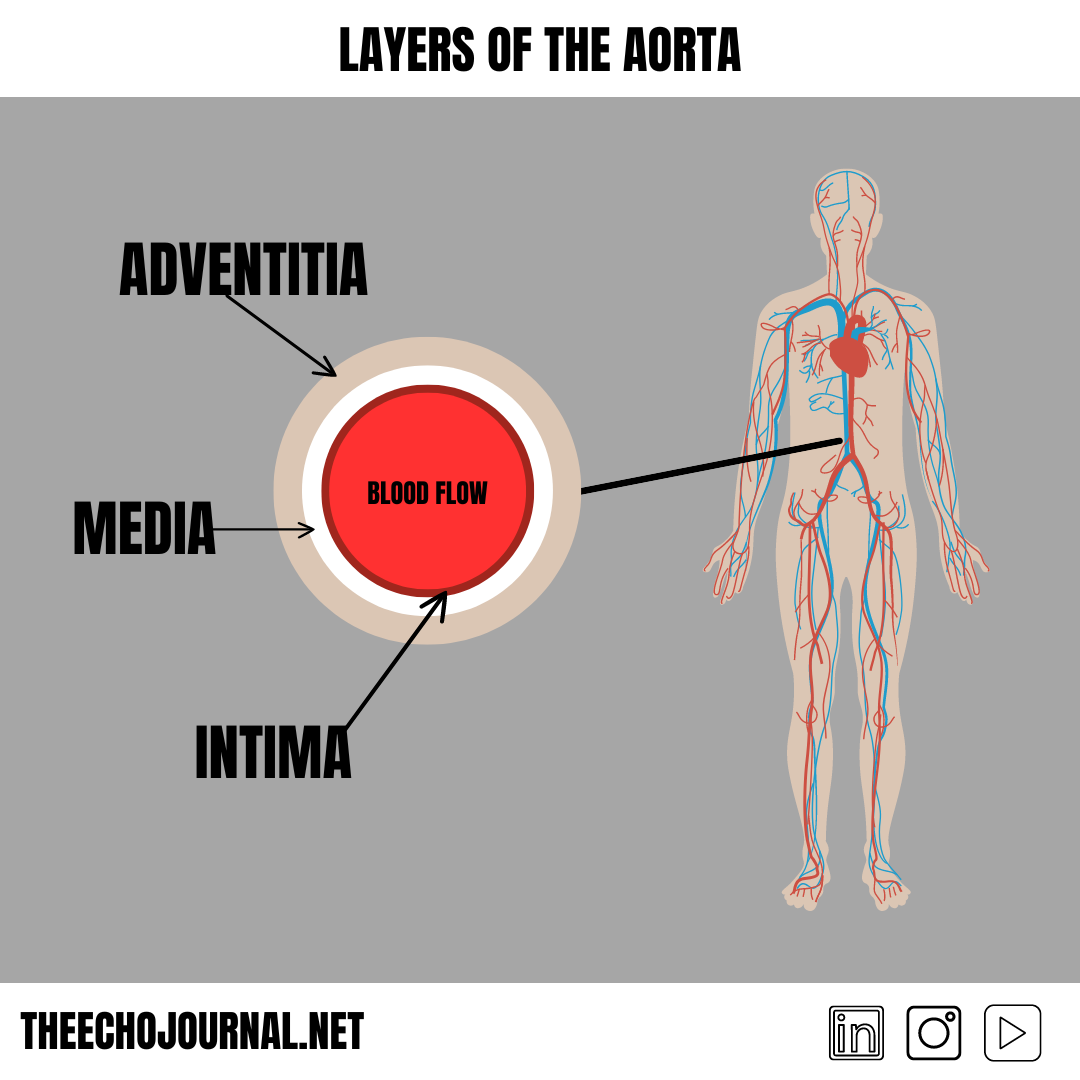
The risk of an AAA is an aortic dissection, a tear in the intimal layer that allows blood to pass between the intima and the media causing them to split. This new flow channel is created and recognition with echocardiography should be thoroughly understood. The key features in this case include: systolic aortic regurgitation, left atrial compression, true and false lumen, and an intimal flap.
The Parasternal Long Axis View
This patient presented to the emergency department with crushing chest pain, altered mental status, and hypotension. A bedside transthoracic echocardiogram was ordered to assess cardiac status. The parasternal long axis view revealed a dilated left ventricular cavity with severely reduced systolic function. What is the origin of this dysfunction? A congestive heart failure exacerbation, dilated cardiomyopathy, significant coronary occlusion, volume overload, or pressure overload are some of the potential causes for this systolic impairment. Join us below in this incredible teaching case example and lesson.
